All published articles of this journal are available on ScienceDirect.

Reverse Hybridization as a Molecular Tool for EGFR Mutation Analysis in Small Biopsies of Lung Cancer
Abstract
Introduction
In recent years, the management of advanced Non–Small-Cell Lung Cancer (NSCLC) has increasingly relied on molecular testing for key driver alterations, particularly Epidermal Growth Factor Receptor (EGFR) mutations and Anaplastic Lymphoma Kinase (ALK) rearrangements. This study aimed to estimate the prevalence of EGFR mutations in NSCLC, characterize the spectrum of EGFR variants across NSCLC subtypes, and compare mutation frequencies between smokers and non-smokers.
Methods
This hospital-based observational study utilized DNA extracted from Formalin-Fixed Paraffin-Embedded (FFPE) tumor samples. Polymerase Chain Reaction (PCR) followed by reverse hybridization was performed using oligonucleotide probe–based EGFR strip assays capable of detecting 16 distinct mutations spanning exons 18–21 of the EGFR gene.
Data analysis was conducted using Microsoft Excel 2013 and SPSS version 17. Associations between EGFR mutation status and clinicopathologic variables were examined using the chi-square test. A p-value < 0.05 was considered statistically significant.
Results
EGFR mutations were identified in 18 cases (66.7%). Among patients with adenocarcinoma, the mutation frequency was 52.6%, whereas all squamous cell carcinoma cases demonstrated EGFR mutations. Within the adenocarcinoma subgroup, EGFR alterations were more frequently observed in females (60%) than in males (50%). Exon 19 in-frame deletions were the most prevalent mutation type detected.
Discussion
The EGFR Strip-Assay represents a sensitive, cost-effective, and less labor-intensive approach with a rapid turnaround time.
Conclusion
This assay may serve as a practical alternative to direct sequencing for EGFR mutation analysis, particularly when working with limited tissue samples in resource-constrained settings such as those in developing countries, including India.
1. INTRODUCTION
Lung cancer is the leading cause of cancer mortality worldwide due to late diagnosis and limited treatment interventions. It has been reported as the second most commonly diagnosed cancer in 2020. In India, 2,54,600 patients were diagnosed with lung cancer in 2020, out of which 1,91,000 (26.4 per 100000) and 63,600 (9.4 per 100000) were males and females, respectively [1].
The diagnosis of lung cancer requires a multidisciplinary approach, including radiological techniques (X-ray and CT Scan), cytopathological evaluation (e.g., sputum and pleural fluid), histopathological evaluation, including Immunohistochemistry (IHC), and molecular evaluation.
The treatment modalities involve surgery (wedge resection, lobectomy, pneumonectomy, etc.), radiotherapy, chemotherapy, targeted drug therapy, and immunotherapy. In recent years, the treatment of patients with advanced NSCLC has been increasingly guided by biomarker testing centered on driver genetic alterations involving the EGFR and ALK rearrangements. The presence of these mutations is predictive of response to targeted therapies such as EGFR Tyrosine Kinase Inhibitors (TKIs) and ALK TKIs [2]. Current guidelines suggest that patients without sensitizing EGFR mutations should not be treated with EGFR TKIs in any line of therapy. The most common EGFR mutation is an in-frame deletion in Exon 19, followed by the L858R mutation in Exon 21. These are termed classic mutations and result in high sensitivity to TKIs. Other EGFR mutations, termed uncommon EGFR mutations, include G719X, S768I, L861Q, Exon 20 insertions, and complex mutations, which are the most frequent. The exon 20 T790M point mutation and most EGFR exon 20ins mutations are predictive of treatment resistance to first- and second-generation EGFR TKI therapies [3].
Limited published data are available regarding EGFR mutation status in the Indian population, especially in the Eastern region. Hence, the study has been undertaken to evaluate the occurrence of EGFR mutations in NSCLC patients by utilizing the EGFR strip assay.
2. MATERIALS AND METHODS
The present study was a hospital-based-observational study conducted at a tertiary care hospital in eastern India from January 2020 to March 2022. Patients of NSCLC diagnosed with IHC with or without clearly evident morphological patterns (adenocarcinoma, squamous cell carcinoma, non-small cell carcinoma favor adenocarcinoma, non-small cell carcinoma favor squamous cell carcinoma, non-small cell carcinoma not otherwise specified) irrespective of age, sex, and smoking habit were included in the study after obtaining written informed consent from each of them. The study followed the Sex and Gender Equity in Research guidelines (SAGER) to ensure appropriate inclusion and reporting of sex-related data.
Patients who have been diagnosed with metastatic carcinoma of the lung, patients with prior tyrosine kinase inhibitor therapy, and patients not willing to participate were excluded from the study.
Relevant clinical history was obtained, and clinical examination was performed. Radiological investigations (X-ray, CT Scan) were recorded, and T staging was noted for each patient.
The CT-guided core-needle biopsy samples were first fixed in 10% neutral buffered formalin and processed in an automated tissue processor (Tissue-Tek®). 10 µm sections were cut from a Formalin-Fixed Paraffin-Embedded (FFPE) tissue block and stained with H&E stain. IHC was performed using a standard IHC protocol according to an automated IHC station, Leica Bond Max®. The following IHC markers and clones were used:
(a) Cytokeratin 7 – Mouse Monoclonal Antibody: OV-TL 12/30
(b) Cytokeratin 20 – Mouse Monoclonal: ks20.8
(c) TTF-1 – Mouse Monoclonal Antibody: (8G7G3/1)
(d) Napsin A – Mouse Monoclonal Antibody: (NAPSA/1238 & NAPSA/1239)
(e) p40 – Mouse Monoclonal Antibody: BC28
2.1. EGFR Mutation Detection with EGFR XL Strip Assay®
Cases showing features of NSCLC on histopathological evaluation were selected for EGFR mutation detection. From these selected blocks, DNA extraction was performed using the help of QIAamp DNA Tissue Kit, followed by DNA quantification on a fluorometric platform (Invitrogen Qubit-4 using the Qubit dsDNA Assay Kit). Next, DNA amplification was performed by Polymerase Chain Reaction (PCR) using biotinylated primers in the Rotor-Gene Q (QIAGEN).
The following PCR programme was used:
(1) Pre-PCR: 37°C/10 min followed by 94°C /2 min.
(2) Thermocycling: 94°C/15sec. - 70°C /60 sec. -58°C /90 sec. (33 cycles)
(3) Final extension: 60°C/3 min.
After amplification, the amplified DNA was stored at 2-8°C.
In the next step, agarose gel electrophoresis was performed on the amplified DNA using SYBR SAFE® as a DNA stain. Electrophoresis was performed in a Wide Mini-Sub Cell GT of BIO-RAD.
The following fragment length was supposed to be visible:
(a) 107,140-149,204 bp in amplification product A [proprietary product]
(b) 90,107,133,147 bp in amplification product B [proprietary product]
After agarose gel electrophoresis, the amplification products were hybridized to ViennaLab StripAssay® test strips. Allele-specific oligonucleotide probes were immobilized as an array of parallel lines on test strips. Amplified DNA was added to bound biotinylated sequences, and it was detected using streptavidin-alkaline phosphatase and color substrates. The strip assay used in this study has an analytical sensitivity of 1% and a concordance rate of 100% with Sanger sequencing [4]. Allele-specific oligonucleotide probes were immobilized as an array of parallel lines on test strips. This assay covered 30 mutations in the EGFR gene (3 in exon 18, 24 in exon 19, 1 in exon 20, and 2 in exon 21) (Fig. 1).
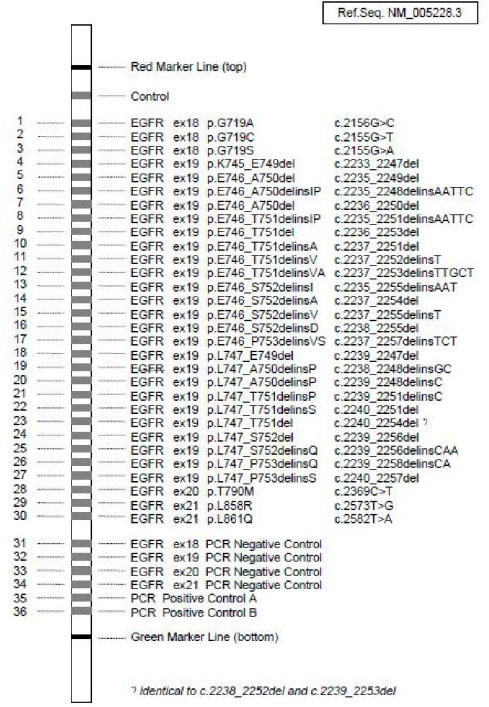
EGFR mutations covered by EGFR XL strip assay.
3. RESULTS
In the present study, a total of 39 cases were included as per the inclusion criteria. However, six cases were excluded due to lack of adequate tissue in the block; five cases were excluded after extraction of DNA due to a DNA quantity below the minimum recommended level of DNA. Further, one case was excluded after PCR due to the absence of any amplified DNA band in DNA agarose gel electrophoresis.
Hence, the total number of cases in which EGFR mutation status evaluation could be conducted was 27. Among these patients, 19 showed features of adenocarcinoma while 8 cases were of squamous cell carcinoma based on immunohistochemistry with or without corroborative histomorphological patterns.
The majority of cases were in the 60-69 years age group, with adenocarcinoma being 47% (9/19) while squamous cell carcinoma was 50% (4/8). This was followed by the age group of > 70 years, wherein adenocarcinoma cases were 31.6% (6/19) and squamous cell carcinoma was 37.5% (3/8). Patients with tumors harboring an EGFR mutation were predominantly > 60 years of age (50-59 years: 14.3%, 60-69 years: 57.1%, > 70 years: 28.6%). Figure 2 shows the age distribution of the study population according to histomorphology.
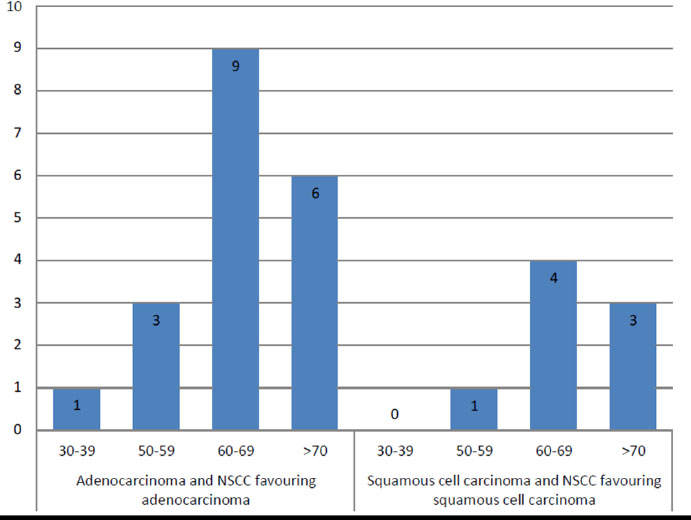
Distribution of study population according to age and histology of tumor.
In the present study, male patients constituted 77.77% (21/27), and 22.23% (6/27) were females.
All female patients were homemakers, while 19% (4/21) of male patients were factory workers and 8.5% (2/21) were farmers. The rest of the male patients had no specific history of occupational exposure.
The history of smoking was present in approximately 60% of the study population (16/27). Smoking was associated with 47.4% (9/19) of patients with adenocarcinoma, whereas 87.5% (7/8) of patients with squamous cell carcinoma were smokers.
66.7% (18/27) of patients expressed EGFR mutation. 77.8% (14/18) of them were males, while the remaining 22.2% (4/18) were females. 66.7% (12/18) of them were smokers, while the remaining 33.3% (6/18) were non-smokers. 78.6% (11/14) of male patients expressing EGFR mutation were smokers, while in female patients, 25% (1/4) were smokers. Table 1 presents the distribution of EGFR mutation among smokers and non-smokers.
| EGFR Mutation | Smokers | Non-smokers |
|---|---|---|
| Present | 12 (66.7%) | 6 (33.3%) |
| Absent | 4 (44.5%) | 5 (55.6%) |
Patients expressing EGFR mutation, 55.6% (10/18) had histological evidence of adenocarcinoma, while 44.4% (8/18) had histological evidence of squamous cell carcinoma.
In patients showing absence of EGFR mutation, 77.8% (7/9) were male while the remaining 22.2% (2/9) were female. 44.5% (4/9) of these patients were smokers while the remaining 55.6% (5/9) were non-smokers. Out of 7 male patients, 4 (57.1%) were smokers.
Among males, EGFR mutation is more common in smokers (73%, 11/15), whereas among females, it is more common in non-smokers (60%, 3/5).
In female patients with absence of EGFR mutation, all were non-smokers. All these patients were diagnosed as adenocarcinoma on histological examination.
Adenocarcinoma was found in 70.4% (19/27) of cases. Among them, 73.7% (14/19) were male, of which 63.3% (9/14) were smokers and 26.3% (5/19) were female. All these females were non-smokers.
EGFR mutation was positive in 52.6% (10/19) of patients diagnosed with adenocarcinoma. Out of these, 70% were male, and 30% were female. About 50% of the patients with the presence of an EGFR mutation were smokers, all being males. Thus, the majority of the male patients with an EGFR mutation were smokers (71.4%).
Patients showing SCC histology constituted 29.6% (8/27) of the study population. 87.5% (7/8) were males, while the remaining 12.5% (1/8) were female. Among them, 85.7% (6/7) of males, as well as the single female patient, were smokers. All these patients expressed EGFR mutation. Table 2 summarizes the distribution of smoking habits according to histology.
| Histology | Smoking Habit Present | Smoking Habit Absent |
|---|---|---|
| Adenocarcinoma with NSCC favoring adenocarcinoma | 9 (44.4%) | 10 (55.6%) |
| Squamous cell carcinoma with NSCC favoring squamous cell carcinoma | 7 (87.5%) | 1 (12.5%) |
EGFR mutation was present in all cases with squamous cell carcinoma and NSCC, favoring squamous cell carcinoma. But in cases of adenocarcinoma or NSCC with a favorable adenocarcinoma histology, EGFR mutation was present in only 52.6% of cases in this study population.
About 50% (5/10) of adenocarcinoma or NSCC with a favorable adenocarcinoma histology in non-smoker were harboring EGFR mutation, while 55.6% (5/9) of adenocarcinoma or NSCC favoring adenocarcinoma in smokers had EGFR mutation.
Therefore, males comprised 70% of cases with adenocarcinoma or NSCC favoring adenocarcinoma showing EGFR mutation, while cases with absence of EGFR mutation were 77.8% male.
In cases of SCC or NSCC favoring SCC expressing EGFR mutation, males were 87.5% of the population.
A single mutation was present in 44.4% (8/18) of all individuals expressing EGFR mutations, and 55.6% (10/18) had complex mutations (> 1 mutation in the EGFR gene). The most common single mutation was Exon 19 deletion (found in 7 cases), followed by a point mutation in Exon 21 (found in only 1 case). The most common Exon 19 deletion mutation was p.L747_P753delinsS(c.2240_2257del), found in all seven cases, while the single case of mutation in Exon 21 was p.L858R(c.2573T>G). Out of 10 cases expressing complex mutations, six cases were having combination of Exon 19 p.L747_P753delinsS(c.2240_2257del) + Exon 21 p.L858R(c.2573T>G), while two cases were having combination of Exon 18 p.G719S(c.2155G>A) + Exon 19 p.L747_P753delinsS(c.2240_2257del) and remaining two cases of complex mutation were having combination of Exon 18 p.G719A(c.2156G>C) + Exon 19 p.L747_P753deli nsS(c.2240_2257del) + Exon 21 p.L858R(c.2573T>G). These findings are summarized in Tables 3-6.
| Study Variables | Exon 19 | Exon 21 | Complex Mutations |
|---|---|---|---|
| Total cases | 7 | 1 | 10 |
| Average age ± SD | 64.6 ± 1.86 | 79 | 65.7 ± 2.6 |
| Male | 6 | 1 | 7 |
| Female | 1 | 0 | 3 |
| Smoking habit present | 4 | 1 | 7 |
| Smoking habit absent | 3 | 0 | 3 |
| Stage: T2 | 4 | 0 | 4 |
| Stage: T3 | 0 | 0 | 4 |
| Stage: T4 | 3 | 1 | 2 |
| Adenocarcinoma+ NSCC favoring adenocarcinoma |
4 | 1 | 5 |
| Squamous cell carcinoma+ NSCC favoring squamous cell carcinoma | 3 | 0 | 5 |
| Exon 18 and 19 | Exon 19 and 21 | Exon 18, 19 & 21 | ||
|---|---|---|---|---|
| Mutation type | Exon 18: p.G719A(c.2156G>C), p.G719S(c.2155G>A) Exon 19: p.L747_P753delinsS (c.2240_2257del) |
Exon 18: p.G717A(c.2156G>C) , p.G719S(c.2155G>A) Exon 19: p.L747_P753delinsS (c.2240_2257del) |
Exon 19: p.L747_P753delinsS (c.2240_2257del) Exon21: p.L858R(c.2573T>G ) |
Exon 18: p.G719A(c.2156G> C) Exon 19: p.L747_P753delinsS (c.2240_2257del) Exon 21: p.L858R(c.2573T> G) |
| Male | 1 | 1 | 4 | 1 |
| Female | 0 | 0 | 2 | 1 |
| Smoker | 1 | 1 | 4 | 1 |
| Non- smoker | 0 | 0 | 2 | 1 |
| Stage: T2 | 0 | 0 | 2 | 2 |
| Stage: T3 | 1 | 1 | 2 | 0 |
| Stage: T4 | 0 | 0 | 2 | 0 |
| Adenoca. + NSCC Favouring adenoca. |
0 | 1 | 2 | 2 |
| SCC+ NSCC Favouring SCC |
1 | 0 | 4 | 0 |
|
Total Number of Patients |
27 | |
|---|---|---|
| Mean Age (Years) | - | 65.26 ±5.6 |
| Gender | Male | 21 (77.8%) |
| Female | 6 (22.2%) | |
| Smoking Status | Smokers | 16 (59.3%) |
| Non-Smokers | 11 (40.7%) | |
| Histopathology | Adenocarcinoma and NSCC Favouring Adenocarcinoma | 19 (70.4%) |
| Squamous Cell Carcinoma and NSCC Favoring Squamous Cell Carcinoma |
8 (29.6%) | |
| Stage T2 | 11 (40.7%) | - |
| Stage T3 | 6 (22.2%) | - |
| Stage T4 | 10 (37.1%) | - |
| EGFR Mutation Status | Mutation Positive | 18 (66.7%) |
| Mutation Negative | 9 (33.3%) | |
| Type of EGFR Mutation | Exon 19 In-frame deletion | 7 (39%) |
| Exon 21 point mutation | 1 (5.5%) | |
| Double mutation in Exon 19 and 21 | 6 (33.3%) | |
| Double mutation in Exon 18 and 19 | 2 (11.1%) | |
| Triple mutation in Exon 18, 19 and 21 | 2 (11.1%) |
| Cases | Age | Gender | Smoking Habit | Egfr Mutation | Exon | Mutation Type |
|---|---|---|---|---|---|---|
| Case 1 | 72 | Male | Present | Absent | - | - |
| Case 2 | 62 | Female | Absent | Absent | - | - |
| Case 3 | 51 | Male | Present | Present | 19, 21 | p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) |
| Case 4 | 62 | Male | Present | Present | 19 | p.L747_P753delinsS(c.2240_2257del) |
| Case 5 | 79 | Male | Present | Present | 21 | p.L858R(c.2573T>G) |
| Case 6 | 56 | Male | Present | Present | 19 | p.E746_A750del(c.2236_2250del) p.L747_P753delinsS(c.2240_2257del) |
| Case 7 | 67 | Male | Present | Present | 19 | p.L747_P753delinsS(c.2240_2257del) p.E746_T751delinsVA (c.2237_2253delinsTTGCT) |
| Case 8 | 63 | Male | Present | Present | 18, 19 | p.G719A(c.2156G>C) p.G719S(c.2155G>A) p.L747_P753delinsS(c.2240_2257del) |
| Case 9 | 38 | Male | Absent | Absent | - | - |
| Case 10 | 71 | Male | Present | Absent | - | - |
| Case 11 | 64 | Male | Absent | Absent | - | - |
| Case 12 | 68 | Female | Absent | Present | 19, 21 | p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) |
| Case 13 | 74 | Female | Present | Present | 19, 21 | p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) |
| Case 14 | 81 | Female | Absent | Absent | - | - |
| Case 15 | 65 | Male | Absent | Present | 19 | p.E746_A750del(c.2236_2250del) |
| Case 16 | 51 | Male | Absent | Absent | - | - |
| Case 17 | 74 | Male | Present | Present | 19, 21 | p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) |
| Case 18 | 70 | Male | Present | Present | 19 | p.L747_P753delinsS(c.2240_2257del) |
| Case 19 | 66 | Male | Absent | Present | 19, 21 | p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) |
| Case 20 | 66 | Male | Present | Absent | - | - |
| Case 21 | 60 | Male | Present | Present | 18, 19 | p.G717A(c.2156G>C) p.G719S(c.2155G>A) p.L747_P753delinsS(c.2240_2257del) |
| Case 22 | 57 | Female | Absent | Present | 18, 19, 21 | p.G719A(c.2156G>C) p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) |
| Case 23 | 71 | Female | Absent | Present | 19 | p.L747_P753delinsS(c.2240_2257del) |
| Case 24 | 69 | Male | Present | Absent | - | - |
| Case 25 | 61 | Male | Present | Present | 19 | p.L747_P753delinsS(c.2240_2257del) |
| Case 26 | 79 | Male | Present | Present | 18, 19, 21 | p.G719A(c.2156G>C) p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) present |
| Case 27 | 65 | Male | Present | Present | 19, 21 | p.L747_P753delinsS(c.2240_2257del) p.L858R(c.2573T>G) |
Complex mutations were present in 50% of males and 75% of females. Complex mutations were more common in smokers, 58.3% (7/12) compared to 50% (3/6) in non-smokers. Patients with complex mutations presented with higher T stage in 60% (6/10) of cases, whereas 50% (4/8) of the individuals harboring a single mutation presented with higher T stage. 50% of patients with adenocarcinoma histology harboring an EGFR mutation were having single mutation, while the rest were having complex mutation. 37.5% of patients with squamous cell carcinoma histology harboring an EGFR mutation were having single mutation, and 62.5% were having complex mutation.
Table 4 shows the distribution of complex mutations in the study population, and Tables 5 and 6 summarize cases according to different study variables.
3.1. Statistical Analysis
In the present study, squamous cell carcinoma was found to be associated with smoking (chi-square value was 3.89 > critical value of chi-square with p = 0.05). In contrast, EGFR mutation was found to be statistically significant in squamous cell carcinoma (chi-square value was 5.8 > critical value of chi-square with p = 0.05). Association between smoking and EGFR mutation was not statistically significant (chi-square value was 1.166 < critical value of chi-square with p = 0.05).
4. DISCUSSION
This study evaluates the prevalence and spectrum of EGFR mutations in NSCLC patients from Eastern India and examines their clinicopathological correlates. EGFR mutations were identified in 66.7% of the cohort, with 52.6% of adenocarcinomas harboring alterations. Geographic heterogeneity in EGFR prevalence is consistent with prior data: approximately 11% in Europeans, 15–20% in Americans, and 35–55% in East Asians; Indian series report 24–52% across regions [5, 6]. Detection rates are influenced by assay methodology: while direct sequencing is a reference method, its analytical sensitivity is limited. This study used a mutant-enriched PCR with reverse hybridization (EGFR Strip-Assay), which offers improved sensitivity.
Among adenocarcinoma or NSCC favoring adenocarcinoma, 50% of non-smokers were EGFR-positive, aligning with Nakra et al. (49%) and comparable to Asian non-smokers in Shi et al. (60.7%) [2, 7]. Notably, 55.6% of smokers carried EGFR mutations, exceeding the 29% reported by Nakra et al. and higher than Shi et al.’s rates for regular (37.3%), ex- (43.2%), and occasional (51.6%) smokers [2, 7]. These differences likely reflect the small sample size and male predominance.
A total of 29.6% of the cohort had squamous cell carcinoma or NSCC favoring squamous histology, and all such cases were EGFR-mutant, markedly higher than the 4–30% reported elsewhere (e.g., Chang et al., Ho et al.) [8, 9]. This likely reflects sampling limitations, including under-recognition of adenosquamous carcinoma in small biopsies [10]. EGFR mutations in adenosquamous carcinoma are detected in 15–44% of Asian patients and typically confer TKI responsiveness comparable to adenocarcinoma [11].
EGFR-mutant adenocarcinoma cases demonstrated male predominance (70%), consistent with Nakra et al. [7]. However, mutation frequency was higher in females (60%) than males (50%), in keeping with previous studies [10, 12]. No significant associations were observed between mutation complexity (single vs. complex) and age, sex, smoking status, or T stage, consistent with Kim et al. [13].
The most frequent alteration was an exon 19 in-frame deletion (38.9%), including six cases of p.L747_P753delinsS (c.2240_2257del) and one case with dual exon 19 deletions (p.E746_A750del plus p.L747_P753delinsS). The second most common variant was exon 21 L858R (5.6%). These distributions are consistent with Indian cohorts [14–16] and southwest Chinese populations [17]. Comparative datasets report exon 19 deletions in 56.6% and L858R in 27.9% (Nakra et al.), exon 19 deletions in 39.3% and L858R in 27.9% with exon 20 insertions at 3.2% (Kim et al., NGS-based), and exon 19 deletions in 32.7% and L858R in 23% in a North American cohort (Robichaux et al.) [7, 13, 18]. The absence of exon 18 (G719X), exon 20 (T790M or insertions), and exon 21 L861Q in the present series likely reflects the Strip-Assay’s limited coverage and the small sample size.
Uncommon mutations (e.g., G719X, S768I, T790M, L861Q, exon 20 insertions) are more readily detected with NGS and appear more prevalent in Asian populations (30–45%) than in American (8–9%) and European (13%) cohorts [9].
Complex EGFR mutations (dual or triple) were observed in 55.6% of cases, substantially exceeding the 6.5% reported by Nakra et al., the 10.2% double mutations reported in Chinese cohorts by Zhou et al., and the 24.6% reported by Kim et al., as well as rates in North American series (Robichaux et al.) [7, 10, 13, 18]. The most common complex pattern combined an exon 19 deletion with exon 21 L858R (60% of complex cases). Two cases harbored combinations involving exon 18 with exon 19 and exon 20 mutations. Exon 20 insertions were not detectable with the current assay, and T790M, often a secondary alteration after TKI therapy, was not identified.
In summary, EGFR mutations were highly prevalent in this Eastern Indian NSCLC cohort, dominated by exon 19 deletions with L858R as the next most frequent variant. The unexpectedly high mutation rate in squamous-predominant tumors likely reflects diagnostic sampling constraints (e.g., under-sampling of adenosquamous carcinoma) and supports confirmatory evaluation on larger specimens when feasible. The high frequency of complex genotypes underscores the utility of comprehensive genomic profiling; broader NGS-based testing would more fully resolve uncommon and compound variants with therapeutic implications.
5. LIMITATIONS
The overall EGFR mutation rate observed in this study (66.7%) and its distribution across histological subtypes 52.6% in adenocarcinomas and 100% in squamous cell carcinomas, deviate from established epidemiological patterns reported in the literature. This represents a key limitation of the present analysis. Potential explanations for this discrepancy include diagnostic misclassification (such as unrecognized adenosquamous carcinoma), the constraints of small or limited biopsy samples, and inherent histopathological challenges that arise in the evaluation of scant tissue.
Additional limitations stem from the inability to perform molecular validation using alternative platforms such as Next-Generation Sequencing (NGS) or Sanger sequencing, primarily due to infrastructural and financial constraints. Furthermore, the hybridization strip assay employed in this study does not encompass several clinically relevant EGFR mutations, thereby reducing its diagnostic and therapeutic utility.
The study’s limited sample size, short duration, and reliance on biopsy-derived material restrict the generalizability of the findings. Because the assay used targets only known mutations, it lacks sensitivity for detecting low-frequency or novel variants, particularly those within exon 20. A larger, more comprehensive investigation incorporating NGS-based approaches is warranted to define the spectrum of EGFR mutations more accurately and to clarify their clinicopathological associations within the Indian population.
CONCLUSION
This hospital-based observational study provides insight into the EGFR mutation profile in NSCLC patients from Eastern India. The EGFR Strip-Assay proved to be a sensitive, cost-effective, and rapid alternative to direct sequencing, especially suitable for limited tissue samples in resource-constrained settings. Early identification of EGFR mutations can significantly impact therapeutic decisions and improve patient outcomes.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| NSCLC | = Non-Small Cell Lung Carcinoma |
| EGFR | = Epidermal Growth Factor Receptor |
| ALK | = Anaplastic Lymphoma Kinase |
| FFPE | = Formalin-Fixed Paraffin-Embedded |
| PCR | = Polymerase Chain Reaction |
| IHC | = Immunohistochemistry |
| CT | = Computed Tomography |
| TKI | = Tyrosine Kinase Inhibitor |
| NGS | = Next-Generation Sequencing |
| H&E | = Hematoxylin and Eosin |
| TTF-1 | = Thyroid Transcription Factor-1 |
| SCC | = Squamous Cell Carcinoma |
| NSCC | = Non-Small Cell Carcinoma |
| DNA | = Deoxyribonucleic Acid |
| bp | = Base Pairs |
| SD | = Standard Deviation |
| T stage | = Tumor Stage (TNM Classification) |
| G719A/S | = Specific EGFR exon 18 point mutations |
| L747_P753delinsS | = EGFR exon 19 deletion-insertion mutation |
| L858R | = EGFR exon 21 point mutation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study is approved by the Institute Ethics Committee meeting of ESI Post Graduate Institute of Medical Sciences and Research, Manicktala, Kolkata, India No. ESI-PGIMSR/MKT/IEC/2020/05 on 15th January 2020.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data of current study are available from corresponding author, [B.D.], on a reasonable request.
ACKNOWLEDGEMENTS
Declared none.

